Stay Informed
Follow us on social media accounts to stay up to date with REHVA actualities

The history of indoor environment begins 1,5 million
years ago when early humans began using campfires. At some point the campfire
was brought inside caves and huts. The oldest arrangement was a central fire
and a central roof opening for smoke to escape. Later the fire was moved to
different parts of a dwelling and various schemes were tried to improve the
efficiency of the fire by using stones. However, even the best open fire was
only 20% efficient considering that most of the heat escaped with the smoke.
Open fireplace heating was used as early as the 800s BC and became widespread
across Europe by the 13th century. Romans
already had underfloor heating to make the indoor climate in their palaces and
spas comfortable (Figure 1). The next important advance
in heating which had influence on thermal comfort was the invention of the
chimney in the 15th century. It took the next
200 years to be widely adopted. The first freestanding warm air stoves were
produced in the 17th century.[1]

Figure 1. The Hypocaustum. Romains system of underfloor heating
Throughout history, man understood that polluted air could be harmful to health. Greeks and Romans were aware of the adverse effects of polluted air in, e.g., crowded cities and mines (Hippocrates, 460–377 BC). Throughout the medieval era, small steps forward have been done in this field. Bad air was held responsible for the spread of diseases and for the unpleasant sensations that were experienced in poorly ventilated rooms. Around 1700, the general idea was that breathing was primarily a way of cooling the heart. But it was also common knowledge that expired air was unfit for breathing until it had been refreshed. [2]
The role of oxygen in breathing was pointed out by Lavoisier (1781), even though Boyle (1627–1691), and Hooke (1635–1703) 100 years earlier (1667) had found that the supply of air to the lungs was essential for life. The work of Antoine Lavoisier (1743– 1794) was especially important for understanding the human metabolism, including the quantitative association between oxygen consumption and carbon dioxide (CO2) release. During the following half century it was accepted that the concentration of CO2 was a measure of whether the air was fresh or stale. [2]
In 1853 Max J. Pettenkofer (1818–1901) – the first professor in hygiene in Munich - noted that the unpleasant sensations of stale air were not due merely to warmth or humidity or CO2 or oxygen deficiency, but rather to the presence of trace quantities of organic material exhaled from the skin and the lungs. He stated that ‘bad’ indoor air did not necessarily make people sick but that such air weakened the human resistance against agents causing illness. In Pettenkofer’s view CO2 was not important but was an indicator of the amount of other noxious substances produced by man. Pettenkofer stated that air was not fit for breathing if the CO2 concentration (with man as the source) was above 1000 ppm and that good indoor air in rooms where people stay for a long time should not exceed 700 ppm, in order to keep the people comfortable. [2]
The first estimate of the required minimum amount of ventilation air was published in 1836 by a Cornish mining engineer Thomas Tredgold. He calculated that one person needed 2 l/s of fresh air for breathing and candle burning. [3]
ASHRAE recommended in 1895
as a minimum rate for ventilation 15 l/s per person. This ventilation rate
was based on the work of John Billings (1836-1913), medical doctor and the American
authority in the field of ventilation at that time.
For several centuries, there were two schools of thought with respect to ventilation. Architects and engineers were concerned with providing comfort, absence of noxious odors and carbon dioxide accumulation. Physicians, on the other hand, were concerned with minimizing the spread of disease. [3]
Possibly the most complete overview of the relationship between indoor environment & health had Florence Nightingale (1820–1910). According to Wikipedia she was 'an English social reformer and statistician, and the founder of modern nursing'. According to Chris Iddon she was 'nurse & structural engineer' [4]. Nightingale (Figure 2) wrote the first modern handbook for the nursing of sick ‘Notes on Nursing, What It Is, and What It Is Not’ [5]. In her foreword she wrote that her book was meant as 'tips for women who are personally responsible for the health of others'.

Figure 2. Florence Nightingale
The first chapter of her book focuses not on patient care, but on ventilation. She wrote: ‘The first task of nursing: to keep the air that breathes the patient as pure as the outside air, without cooling them.’ In the second chapter she mentioned five essential points to ensure the health of houses:
· Pure air
· Clear water
· Efficient waste water drainage
· Hygiene
· Light
Nightingale has seen and approached the problems of the indoor environment in its entirety. Other recommendations from her, which are being rediscovered today, are:
· Bring air from outside. Open your windows and close your doors.
· (Natural) air temperature fluctuations are necessary to stay healthy.
· Light is essential for both health and recovery.
· The body and mind degenerate without sunlight.
In the beginning, thinking about the indoor environment was in the realm of philosophy. Much later, in the 19th century, indoor environment concerns were covered by two separate disciplines: medicine and engineering.
In the 20th century researchers were increasingly convinced that ventilation is mainly a matter of comfort and not of health. There was a growing resistance to heating the large amounts of outside air prescribed for ventilation.
The beginning of the 20th century marks also the birth of air-conditioning, an invention that turned out to have a major impact on the indoor environment. Probably the first building with cooling (without using ice) is the Stock Exchange building in New York, USA. Alfred Wolff (1859–1909) designed the cooling system that used three ammonia absorption chillers, with a cooling capacity of 1,582 kW [6]. Yet he did not become the best-known air-conditioning engineer.
Willis H. Carrier (1876–1950) is known as the inventor (or father) of modern air-conditioning. Carrier designed his first system in 1902 to control temperature and humidity in a printing plant in Brooklyn (New York, USA). Unfortunately, this system did not work well and the design conditions couldn’t be maintained. However, this design is generally marked as the first application of air-conditioning. Since then, air-conditioning has been defined as a system that must have four basic functions:
· Temperature regulation
· Humidity control
· Air circulation and/or ventilation
· Air purification (filtration)
Carrier designed in 1904 a spray-type air-conditioner, a very sophisticated air washer, with which he could control the absolute humidity of the air leaving the conditioner and, ultimately, the relative humidity of the conditioned space. In January 1906, he obtained the patent called 'Apparatus for Treating Air’ [7]. (The term 'air-conditioning' was first coined by the American textile engineer Stuart Cramer).
In 1911 Carrier presented his 'Rationale Psychrometric Formulae' at a meeting of ASHRAE. This became the basis for the fundamental calculations in the air-conditioning industry. His work helps to determine the precise relationship between temperature and humidity in order to be able to regulate the indoor climate throughout the year. With his scientific work, his vision of a new industry – air-conditioning - and with his entrepreneurial activities, Carrier has had a very strong influence on the indoor environment field (Figure 3). However, he was never really involved in comfort-related issues.

Figure 3. An example of air conditioning industry
Leonard Hill (1866–1952) dedicated his life and work to research improving the physical well-being of people. He didn’t find any evidence that high concentrations of CO2 can cause discomfort and, therefore, he concluded that heat and odor (caused by physical emissions) are the main sources of uneasiness in rooms with poor ventilation [8].
Using an instrument known as the 'kata thermometer', he determined the cooling capacity of air movement on the human body. This was used to monitor workplace conditions in the United Kingdom, including the House of Commons, where Hill was concerned that ‘cold feet and stuffy heads result - just the wrong conditions for legislators’ [9].
In 1923, ASHRAE Journal published the article 'Determination of the comfort zone' (Houghten & Yaglou) [10], in which the conditions for comfort were presented on a psychrometric diagram. They used the index 'Effective Temperature' (ET), which was used extensively over the next 50 years [11]. ET is defined as the dry bulb temperature (DBT) of a uniform environment with a relative air humidity of 50%, which would have the same heat exchange, by radiation, convection and evaporation, as the environment in question (Figure 4).
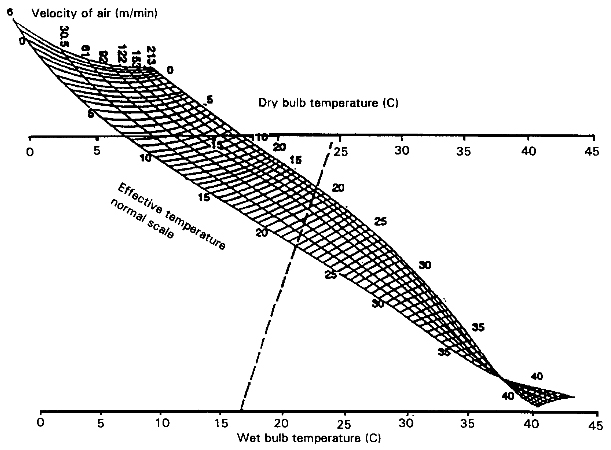
Figure 4. Effective Temperature nomogram (Yaglou)
Constantin Yaglou[1] (1897–1960) also studied the relationship between body odor and ventilation flow. He concluded that these odors are not really harmful to building users and that CO2 concentration cannot be a good indicator of the air quality in buildings. Yaglou noted that odors are probably related to temperature and humidity[12]. Ventilation requirements were measured by using the human nose as a sensor.
In 1936 ASHRAE recommended
7.5 l/s per person on the basis of work of C. Yaglou.
Adolf P. Gagge (1908-1993) introduced his ‘Two-node model’ in 1936. It calculates the thermal response by means of two energy balance equations, one for the core node and one for the skin node. This model (sometimes called Pierce model because Gagge made it together with his colleagues at JB Pierce Laboratories of Yale University) assumes that the sum of the heat exchange between humans and their environment through metabolism, activity, evaporation, radiation and conduction is zero. [13] With his model Gagge applied the first law of thermodynamics (conservation of energy) on man and his environment. [14] This model was expanded later (after World War II.).
Gagge's work helped define the study area of energy exchange between the human body and the immediate environment. It’s application had an impact on health and safety at work, in the military, in space exploration and in the design and operation of buildings [14].
From the early 1960s there were many researchers working in the field of thermal comfort. The most well-known and influential was Povl Ole Fanger (1934–2006). Fanger (Figure 5) focused on the relationship between the physical parameters of the environment, the physiological parameters of people and the perception of comfort expressed by people themselves. In 1970, he published his dissertation 'Thermal Comfort' [15] in which he defined a new discipline: the study of the condition of comfort and well-being in indoor environments. [14] The conceptual leap introduced by Fanger, compared to previous studies, is the introduction of the judgment scale by people themselves.

Figure 5. P. O. Fanger
Using Fanger's comfort theory, it is possible to predict to what extent a certain indoor environment will be experienced by building users as 'cold', 'neutral' or 'warm'. The prediction of the mean thermal sensation, which is associated with a combination of six environmental and personal parameters (air temperature, mean-radiant temperature, relative humidity, air velocity, activity level and thermal resistance of the clothing), is given as 'Predicted Mean Vote' (PMV-index). The PMV-index indicates the predicted opinion of a group of people with identical metabolism and clothing regarding their thermal sensation. It does not predict the acceptability of the environmental conditions (Table 1). As a follow-up to the PMV-index, Fanger introduced the PPD-index (Predicted Percentage of Dissatisfied) that does predict the acceptability (Figure 6). Fanger’s model was developed for the applications in air-conditioned buildings but, from the 1980s, it was also used for other applications (non-air-conditioned rooms). In other words, the interpretation of Fanger's work in practice is not entirely correct [16].
Table 1. Scale of the PMV index. [Source: NEN-EN-ISO 7730]
+3 | Hot |
+2 | Warm |
+1 | Slightly warm |
0 | Neutral |
-1 | Slightly cool |
-2 | Cool |
-3 | Cold |
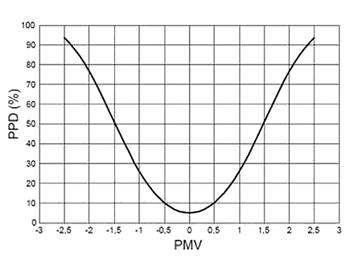
Figure 6. The relationship between PMV and PPD (Fanger)
Environmental aspects largely focused on indoor air quality until the 1960s. In 1962, Rachel L. Carson (1907–1964) wrote her book 'Silent Spring'. In this book she describes the harmful effects of pesticides on the environment. It is widely credited with helping launch the environmental movement. Environment was suddenly synonymous with outside air and industrial environment. Environmental protection received worldwide attention but IAQ (indoor air quality) in non-industrial indoor environments was not on the list of environmental problems.
In 1973, ASHRAE published
its first Standard 62 with the recommended amount of supplied air of 7.5 l/s
per person.
In 1981, ASHRAE divided the
recommended amount of fresh supply air into two categories. For non-smoking
rooms 2 l/s per person and for rooms where smoking was allowed 10 l/s
per person.
Many different studies have shown that indoor air quality is influenced by the quantity and quality of the supplied fresh air, pollution by people themselves and emissions of the materials used in buildings. More and more specific studies have been carried out with regards to radon, tobacco smoke, VOC (volatile organic compounds), formaldehyde, (fine) dust, asbestos, dust mites and other agents that influence the indoor air quality.
With the amount of fresh supply air minimized to 2 l/s per person (as a result of the energy crisis in the 1970s), there were more and more problems with the indoor environment, especially in office buildings (Figure 7). Many different terms were used to indicate the phenomenon of reported high occurrences of health problems and diseases. From 1982, the World Health Organization (WHO) used the term Sick Building Syndrome (SBS) and this became the most commonly used term. SBS relates to a number of symptoms that are experienced by several building occupants when they are in a building and which reduce or disappear completely when they leave the building. Since 1989, Healthy Buildings congresses have been organized to bring researchers from medical sciences together with engineers and technicians from practice to solve the problems that cause SBS.

Figure 7. The overview of the recommended amount of air supply in ASHARE standards (Source: Olesen, 2011: PowerPoint-How much ventilation and how to ventilate in the future)
A major challenge is that research and practice mostly focus on individual components. It is only during the last decades of the twentieth century that the first attempts towards more holistic approaches to indoor environmental problems were made [17]. With the holistic approach of the indoor environment, 'soft' factors are also taken into account. After the decades in which medical doctors and engineers had investigated the problem separately, these disciplines began to learn from each other. In the research on Sick Building Syndrome many psychological studies were conducted which focused on the perception of people. Many buildings are designed in a way that does not connect with evolutionary old 'software' in our brain; i.e., the basic laws that govern our behavior. [18] The relevant laws are:
· People and animals need change. This applies in particular to thermal comfort. A homogeneous environment means that people feel less comfortable.
· Man wants to constantly intervene in his environment. This law also applies mainly to the thermal comfort but also to ergonomics (furniture).
· A meaning must be given to stimuli. For example, a smell that is present in the building and that cannot be recognized, leads to a state of chronic alarm.
· Man always strives to have his own territory. This becomes a problem, for example, in open plan offices.
· Man has been living in artifacts for only several centuries and this has broken his contact with the natural environment. That’s why the view to outside is very important. [18]
The 1980s saw the start of the discussion about adaptive principles related to thermal comfort. The initiator was Michael A. Humphreys. An English physicist who does a lot of research into thermal adaptation of building occupants. In 1998, he wrote together with J. Fergus Nicol, an article ‘Understanding the Adaptive Approach to Thermal Comfort [19]. The starting point of their discussion was: ‘If a change occurs such as to produce discomfort, people react in way that tend to restore their comfort’. They explain adaptation as ‘all those physiological, psychological, social, technological, cultural, or behavioral strategies people might use to try to secure their comfort’. Some other researchers confine the term adaptation to that kind of physiological or psychological acclimatization through which a person might come to prefer or accept a different set of skin temperature or sweat rates for comfort. [19]
Gail S. Brager and Richard J. de Dear published in 1997 a literature study on thermal adaptation in the built environment [20] and developed an adaptive model of thermal comfort [21] (Figure 8). This research was subsequently included in ASHRAE Standard 55. The field studies made it clear that Fanger's PMV-index might be too strict for non-air-conditioned buildings where users themselves could have control over the indoor environment. In other words, where people have the possibility to influence their environment (for example by opening windows).
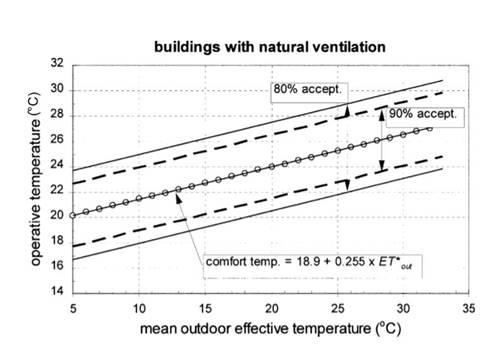
Figure 8. The shift in attention to the three health aims of building services that constitute complete health (Source: reference 22)
From the indoor environment developments during the past three centuries it can be concluded that health had priority in the beginning. In the 18th century people wanted to have a healthy environment in buildings in order to prevent the spread of diseases. Later, the indoor environment problems were dominated by comfort issues [22] (Figure 9). People wanted to be able to realize comfortable indoor conditions throughout the year. After the oil crisis in the 1970s, the main goal was to save as much energy as possible on indoor environment conditioning. Towards the end of the 20th century, sustainability became very important. In the Netherlands, sustainability was primarily seen in the form of fossil energy. For example, Trias Energetica with special attention for energy saving (isolation of buildings) and generation of sustainable energy (use of solar boilers and later PV panels). Only a few years ago (beginning of the 21st century) people regained interest in health in the build environment. New topics regarding indoor environment are being discussed, such as influence of the indoor environment on productivity or supporting health and well-being of building occupants. These are nowadays topics which don’t belong to history yet.
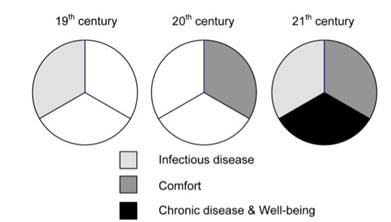
Figure 9. Indoor environment problems dominated by comfort issues.
[1] B.
Nagengast, “An Early History Of Comfort Heating,” ACHRNEWS.com, 2001.
[2] J. Sundell, “On the history of indoor air
quality and health,” Indoor Air, vol. 14, no. 7, pp. 51–58, 2004.
[3] J. E. Janssen, “The History of ventilation
and Temperature Control,” ASHRAE
J., vol. October, pp.
48–70, 1999.
[4] C. Iddon, “Florence Nightingale: nurse and
building engineer,” 2015. [Online]. Available:
http://www.cibsejournal.com/general/florence-nightingale-nurse-and-building-engineer/.
[5] F. Nightingale, Notes on Nursing, What It Is, and What It Is
Not. 1859.
[6] B. Roberts, “ALFRED WOLFF AIR CONDITIONING
PIONEER,” 2014. [Online]. Available:
http://www.hevac-heritage.org/built_environment/pioneers_revisited/wolff.pdf.
[7] B. Nagengast, “Early Twentieth Century
Air-Conditioning Engineering,” ASHRAE
J., no. March, pp. 55–62,
1999.
[8] L. Hill, M. W. Flack, J. McIntosh, R. A.
Rowlands, and H. B. Walker, “The Influence of the atmosphere on our health and
comfort in confined and crowded places,” Smithson. Misc. Collect., vol. 60(23), 1913.
[9] J. Clayton, “Behind the picture: Leonard
Hill and the divers,” 2014. [Online]. Available:
http://www.insight.mrc.ac.uk/2014/08/13/behind-the-picture-leonard-hill-and-the-divers/.
[10] F. Houghten and C. Yaglou, “Determination of
the comfort zone,” ASHVE Trans
29, vol. 29, pp. 165–176,
1923.
[11] A. Auliciems and S. V Szokolay, “Thermal
comfort,” PLEA Notes, p. 66, 2007.
[12] C. P. Yaglou,
“Ventilation Requirements,” ASHVE
Trans., vol. 42, 1936.
[13] A. Gagge, “The linearity criterion as applied
to partitional calorimetry,” Am.
Physiol. Soc., vol. 116,
no. 3, pp. 656–668, 1936.
[14] K. Fabbri, “A Brief History of Thermal
Comfort: From Effective Temperature to Adaptive Thermal Comfort,” in Indoor Thermal Comfort Perception: A
Questionnaire Approach Focusing on Children, 2015, pp. 1–302.
[15] P. Fanger, “Thermal comfort. Analysis and
applications in environmental engineering.,” Therm. Comf. Anal. Appl. …, 1970.
[16] J. Van Hoof, “Forty years of Fanger’s model of
thermal comfort: Comfort for all?,” Indoor Air,
vol. 18, no. 3, pp. 182–201, 2008.
[17] P. M. Bluyssen, The Indoor Environment Handbook, vol. 165, no. 3. 2012.
[18] P. A. Vroom, Psychologischeaspecten van ziekmakendegebouwen. ISOR, 1990.
[19] M. A. Humphreys and J. F. Nicol,
“Understanding the adaptive approach to thermal comfort,” in ASHRAE Transactions, 1998, vol. 104, no. Pt 1B, pp. 991–1004.
[20] G. S. Brager and R. J. De Dear, “Thermal
adaptation in the built environment : a literature review,” Energy Build., vol. 27, pp. 83–96, 1998.
[21] R. De Dear, G. Brager, and C. Donna, “Developing an adaptive model of thermal comfort and preference,” ASHRAE Trans., vol. 104, no. Part 1, pp. 1–18, 1998.
[22] F. Franchimon, “Healthy building services for
the 21st century,” doctoral dissertation, Technische Universiteit Eindhoven,
2009.
Follow us on social media accounts to stay up to date with REHVA actualities
0